Introduction to Nursing Care Plans
A nursing care plan is a written guide that tells a nurse how to care for a patient step by step. It helps organize your thoughts and ensures the patient gets proper treatment.
Why it matters: If your care plan is messy or incomplete, the patient may not get the right care, and you lose marks in assignments. For official nursing standards, see the Nursing and Midwifery Council (NMC UK)

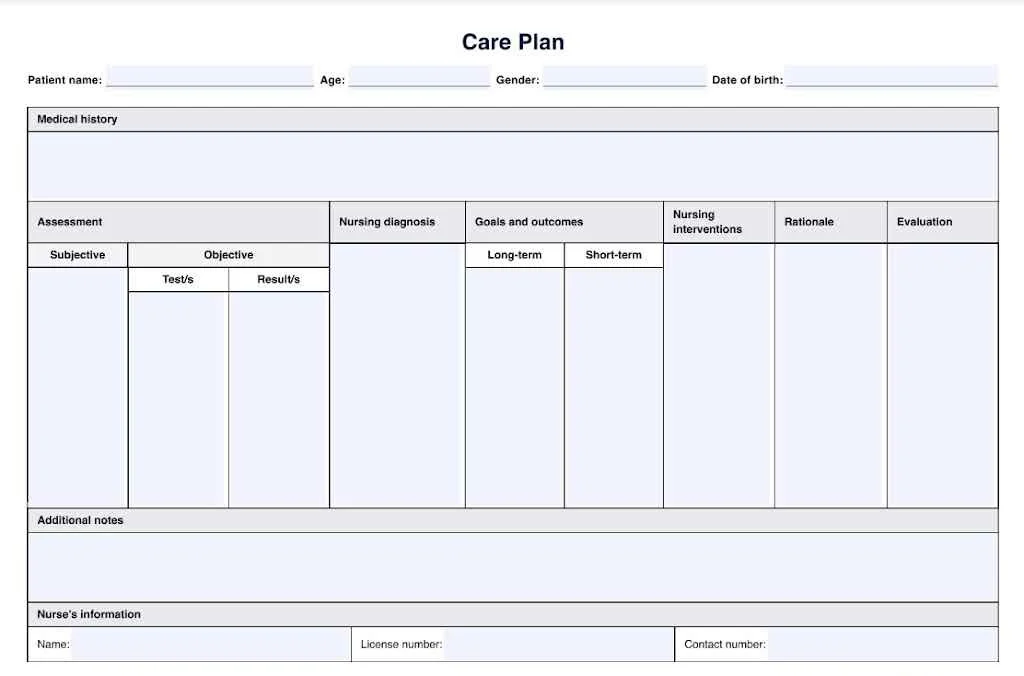
What is a Nursing Care Plan?
A nursing care plan shows what problems the patient has, what the nurse will do, and how to check if it worked.
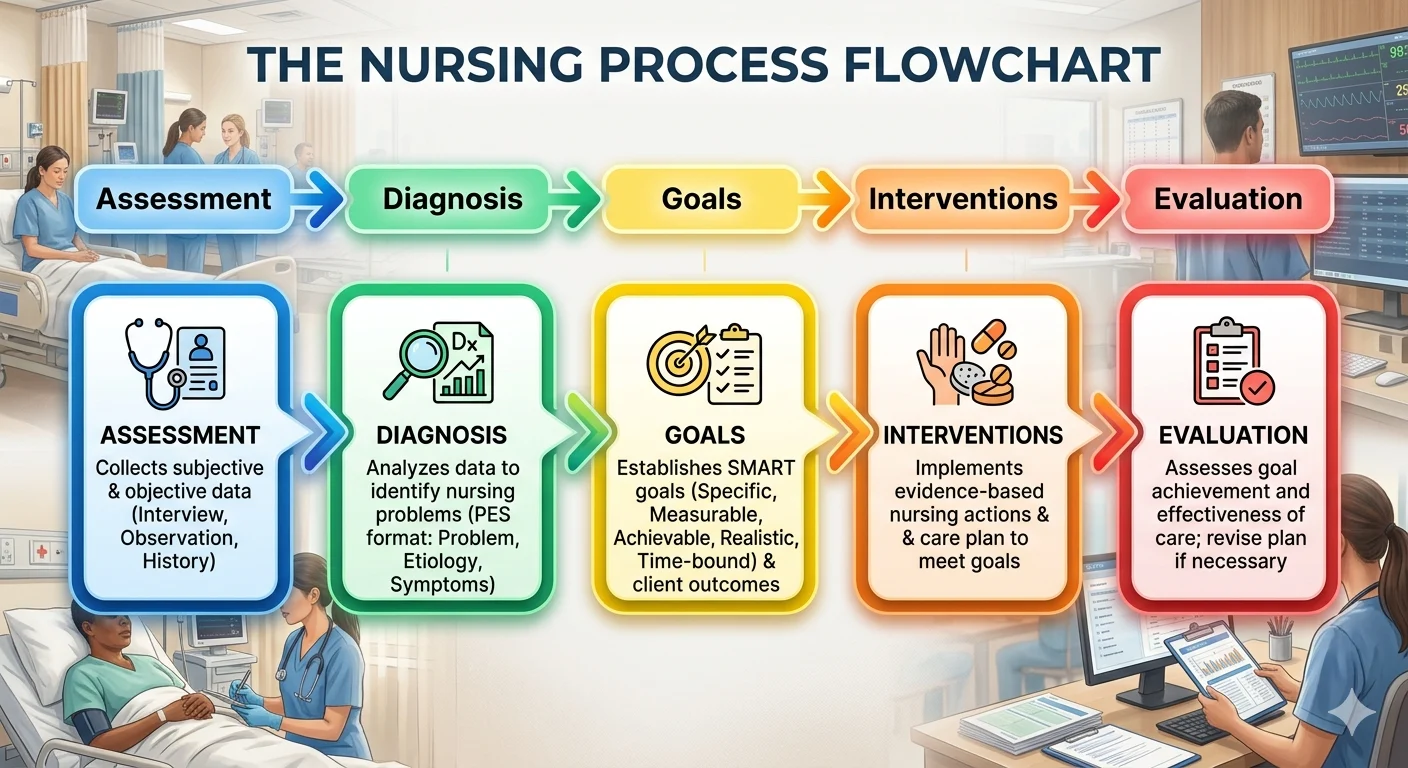
Key parts of a care plan:
- Patient assessment
- Nursing diagnosis
- Goals
- Interventions
- Evaluation
It is a roadmap for nurses to provide consistent, safe, patient-centered care. More on patient-centered nursing care: NHS: Patient Care Guidelines
Why Nursing Care Plans Are Important
Care plans help nurses:
- Understand the patient’s condition
- Plan proper care
- Track improvement
For students, they help develop critical thinking and clinical reasoning skills.

Types of Nursing Care Plans
Formal Care Plan
A formal care plan is detailed and used for assignments and hospitals. It has all sections filled in with explanations.
Informal Care Plan
Used in hospitals for quick thinking. Not usually written down in detail.

Standardized Care Plan
A template for common illnesses like diabetes or high blood pressure. Saves time but not always personalized.
Individualized Care Plan
Tailored to the specific patient. Shows critical thinking. Best for assignments.

Step 1 – Patient Assessment
Assessment is the first step. You collect all the information about the patient.
What to Assess
- Medical history
- Current symptoms
- Vital signs (heart rate, blood pressure, oxygen levels)
- Lab test results
- Mental health
- Family and social situation
For guidelines on respiratory assessment, see NICE Respiratory Guidelines

Example Assessment
A patient has:
- Shortness of breath
- Oxygen level at 89%
- History of COPD
This tells you that breathing is a problem.

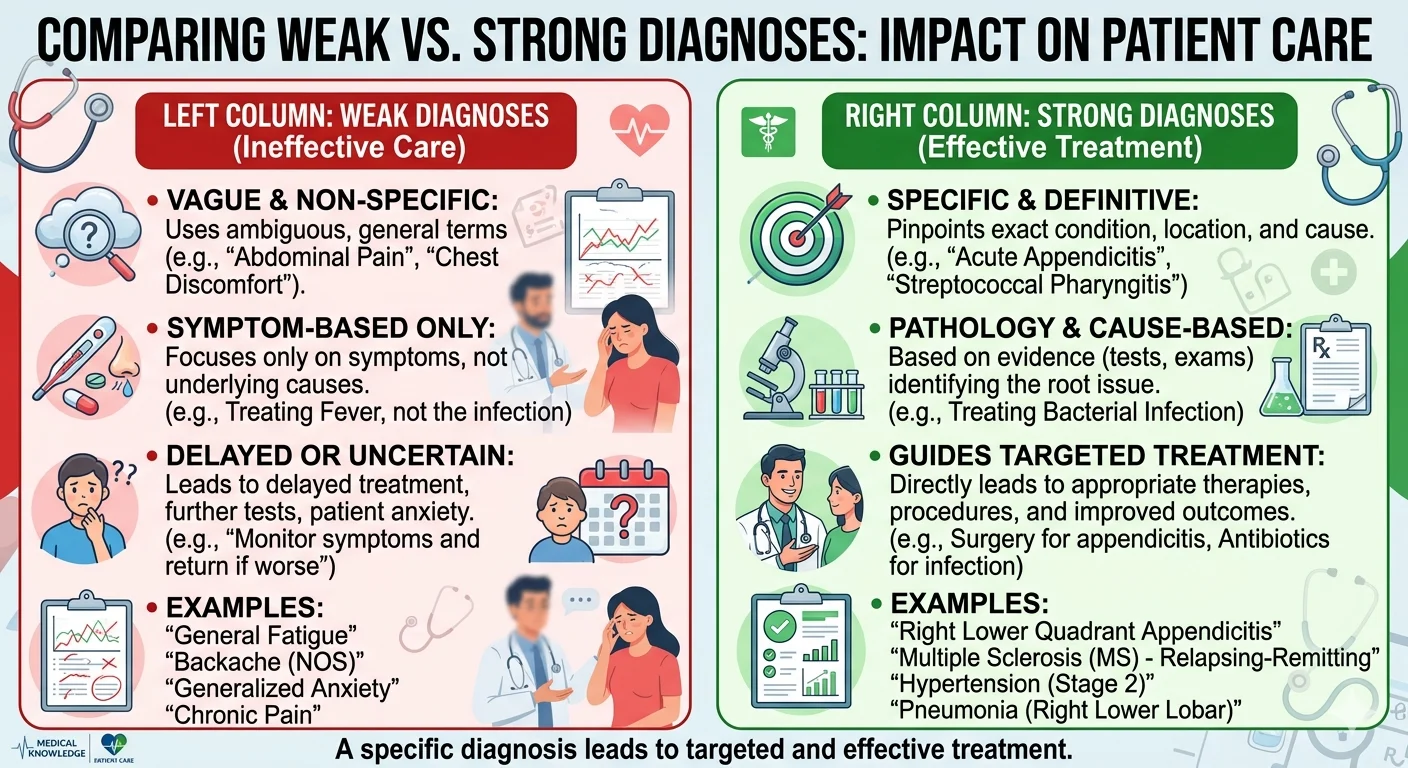
Step 2 – Nursing Diagnosis
A nursing diagnosis identifies problems that nurses can manage.
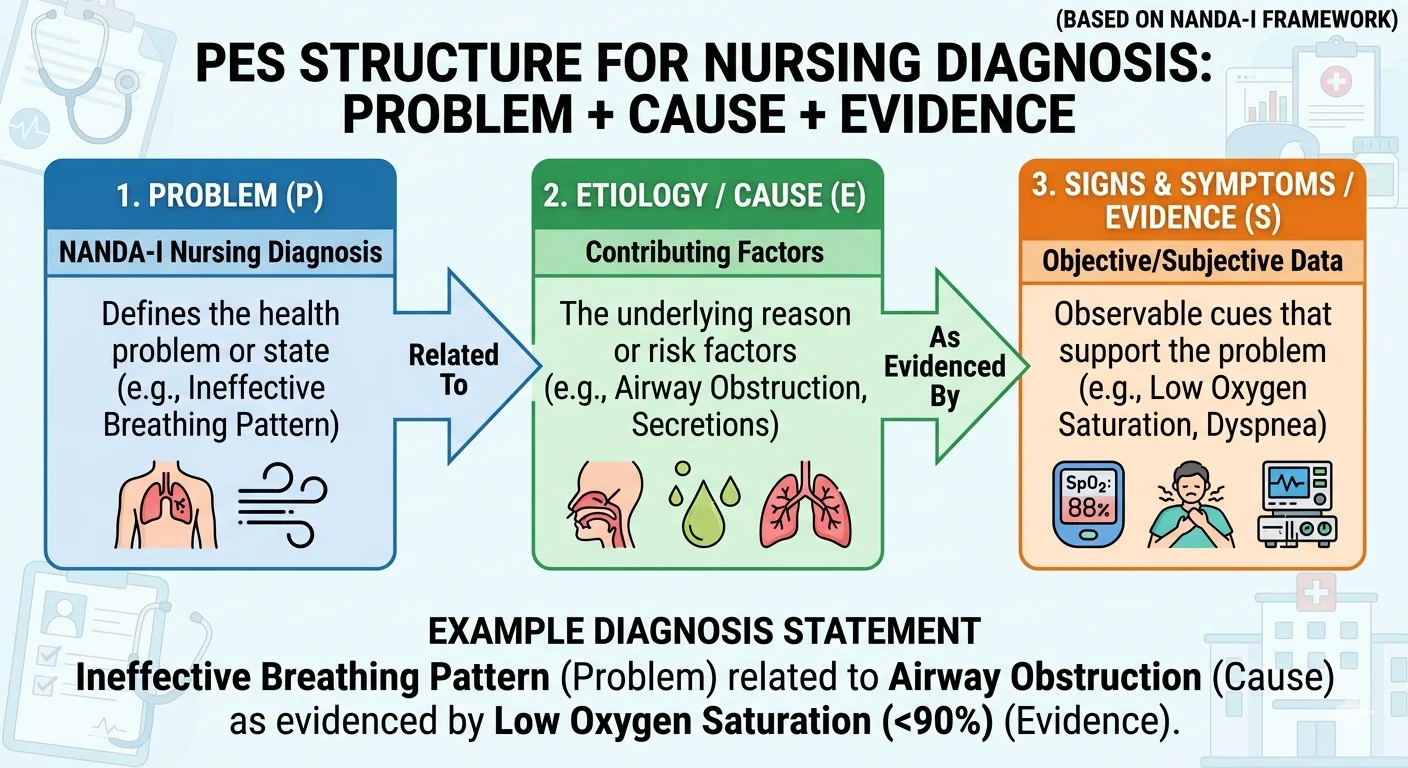
How to Write It
Format: Problem + Cause + Evidence
Example:
Ineffective breathing pattern related to airway obstruction as shown by low oxygen saturation.
For official examples of nursing diagnoses, see NANDA International .
Common Mistakes
- Writing medical diagnoses instead of nursing problems
- Being vague
- Forgetting to link evidence
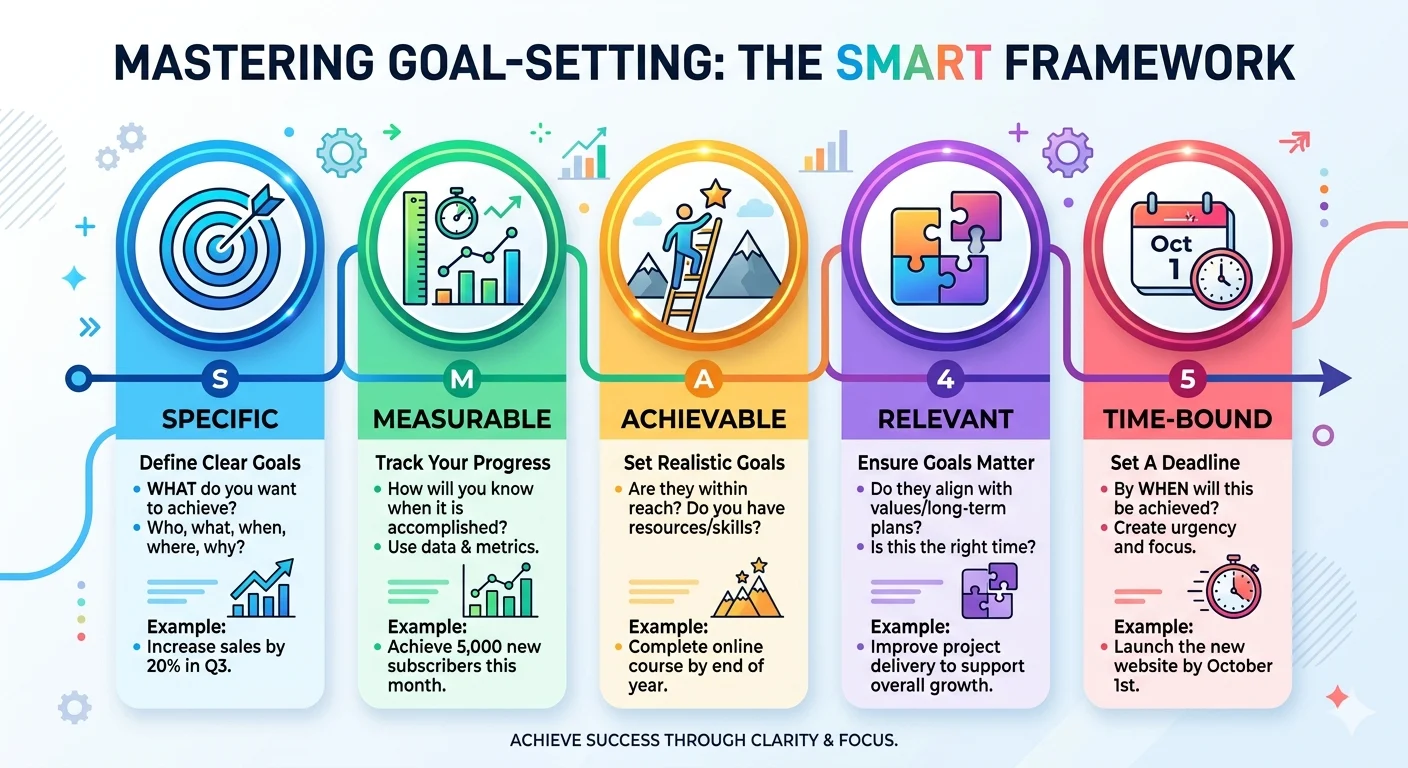
Step 3 – Setting Goals
Goals show what you want the patient to achieve.
SMART Goals
- Specific
- Measurable
- Achievable
- Relevant
- Time-bound
Example: The patient will maintain oxygen saturation above 95% in 24 hours.
Step 4 – Nursing Interventions
Interventions are what the nurse does to help the patient reach the goal.
Types of Interventions
- Independent (nurse can do without doctor)
- Dependent (requires doctor’s order)
- Collaborative (work with other health professionals)
Examples
Position patient in semi-upright position
Monitor oxygen levels every 2 hours
Give oxygen therapy
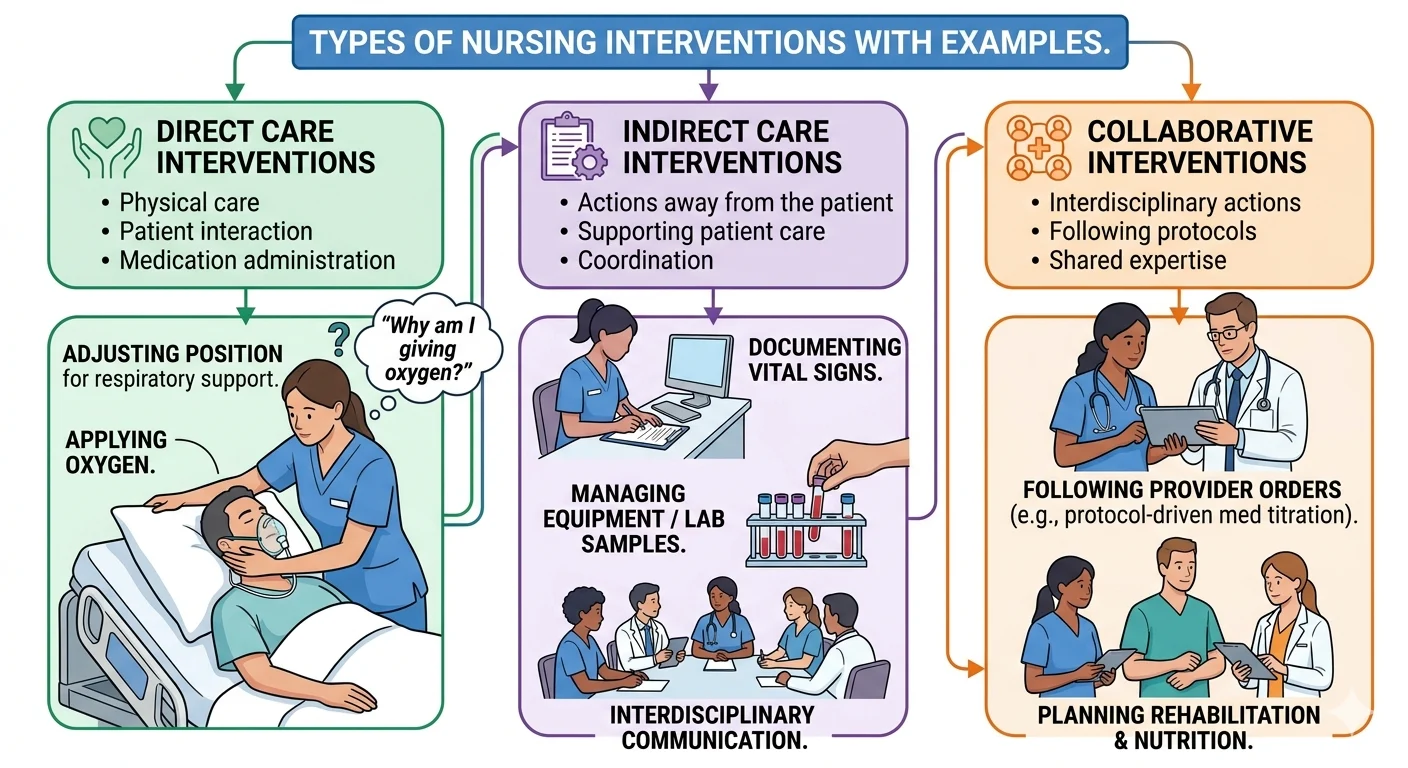
Tip
Always ask yourself: Why am I doing this? See NHS guide for oxygen therapy: NHS: Oxygen Therapy
Step 5 – Rationale
Rationale explains why each action is needed.
Importance
Shows that your decisions are based on knowledge and evidence, not guesses. More on evidence-based nursing: BMJ Evidence-Based Nursing
Example
Monitoring oxygen levels helps detect hypoxia early, so nurses can act quickly.

Step 6 – Evaluation
Evaluation checks if your plan worked.
What to Include
- Did the patient improve?
- Was the goal achieved?
- Any changes needed?
Example: Patient’s oxygen improved to 96%, goal achieved.

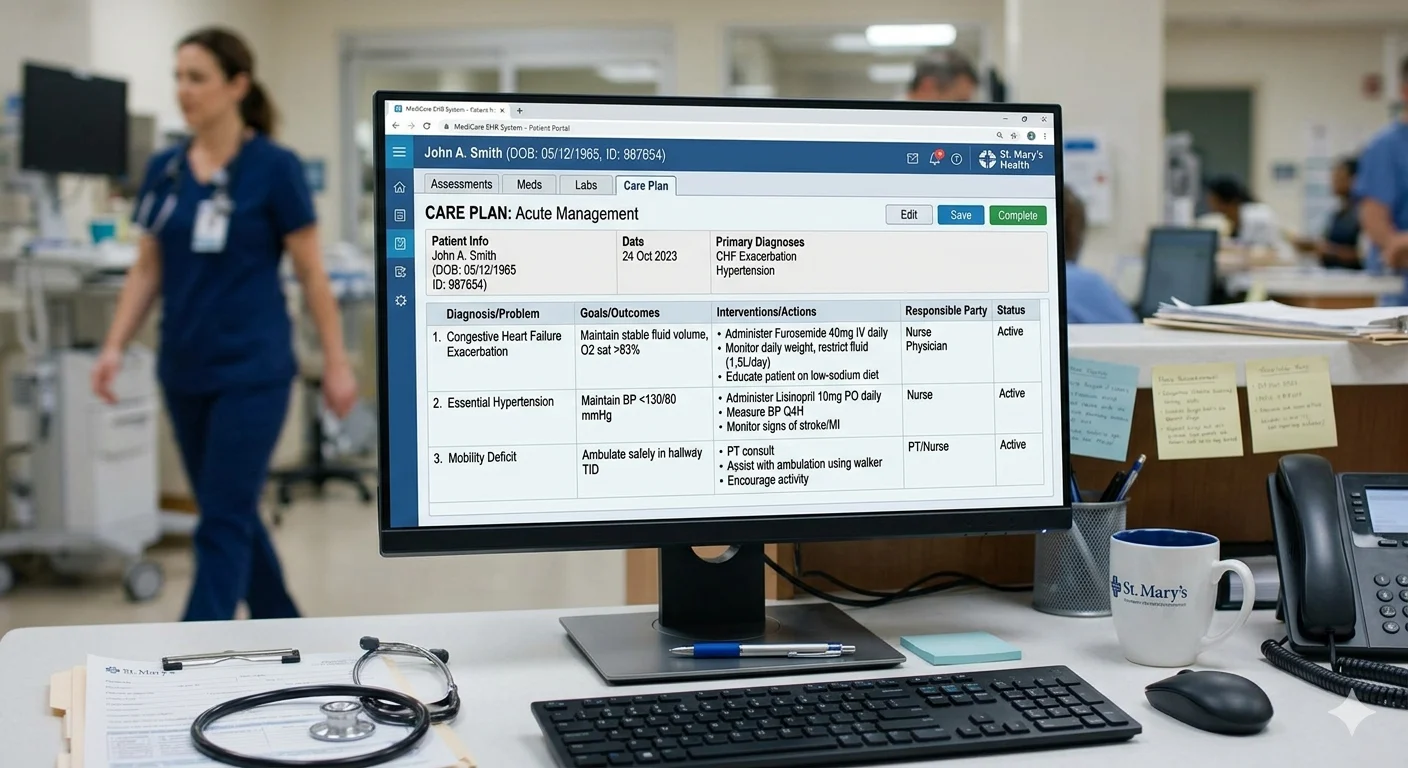
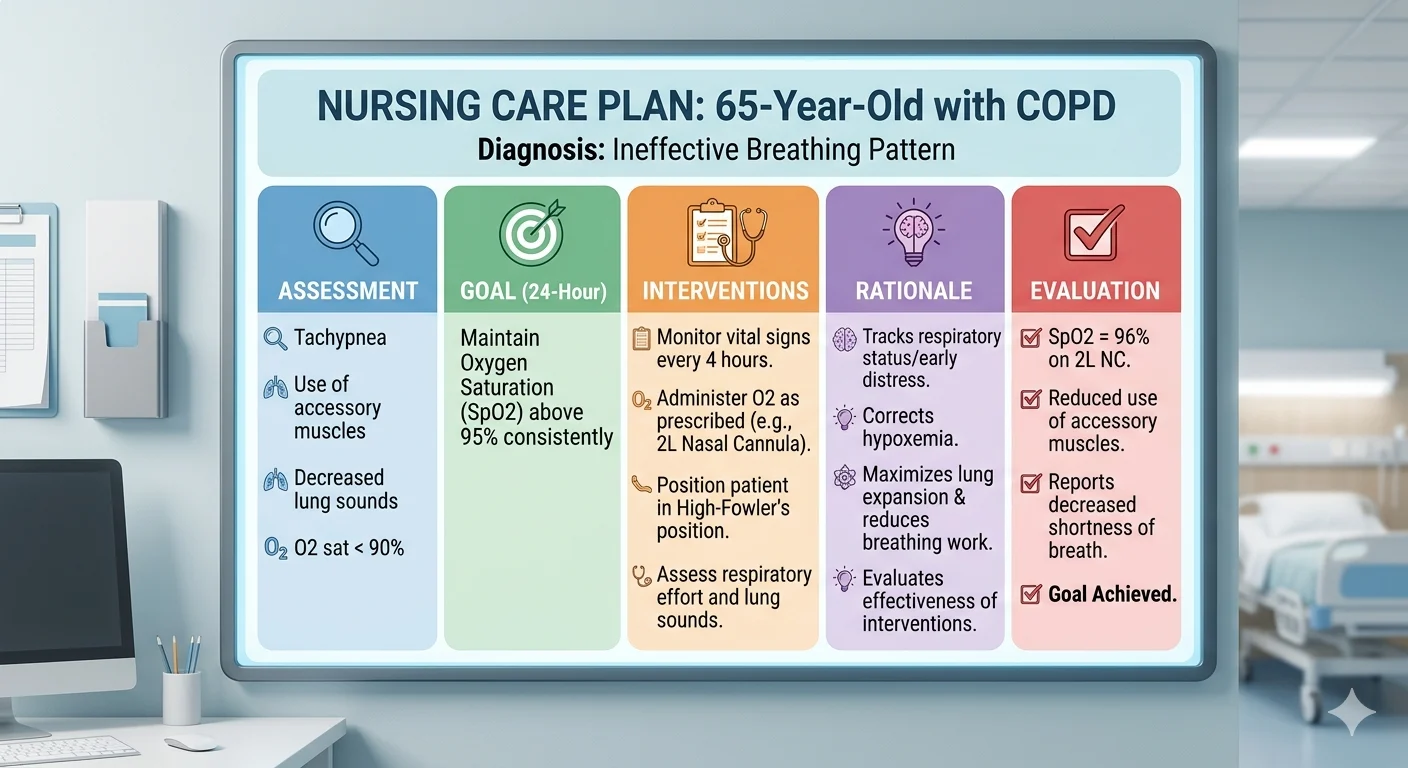
Full Nursing Care Plan Example
Patient: 65-year-old with COPD
Diagnosis: Ineffective breathing
Goal: Oxygen above 95% in 24 hours
Interventions: Monitor vitals, provide oxygen, adjust position
Evaluation: Goal achieved
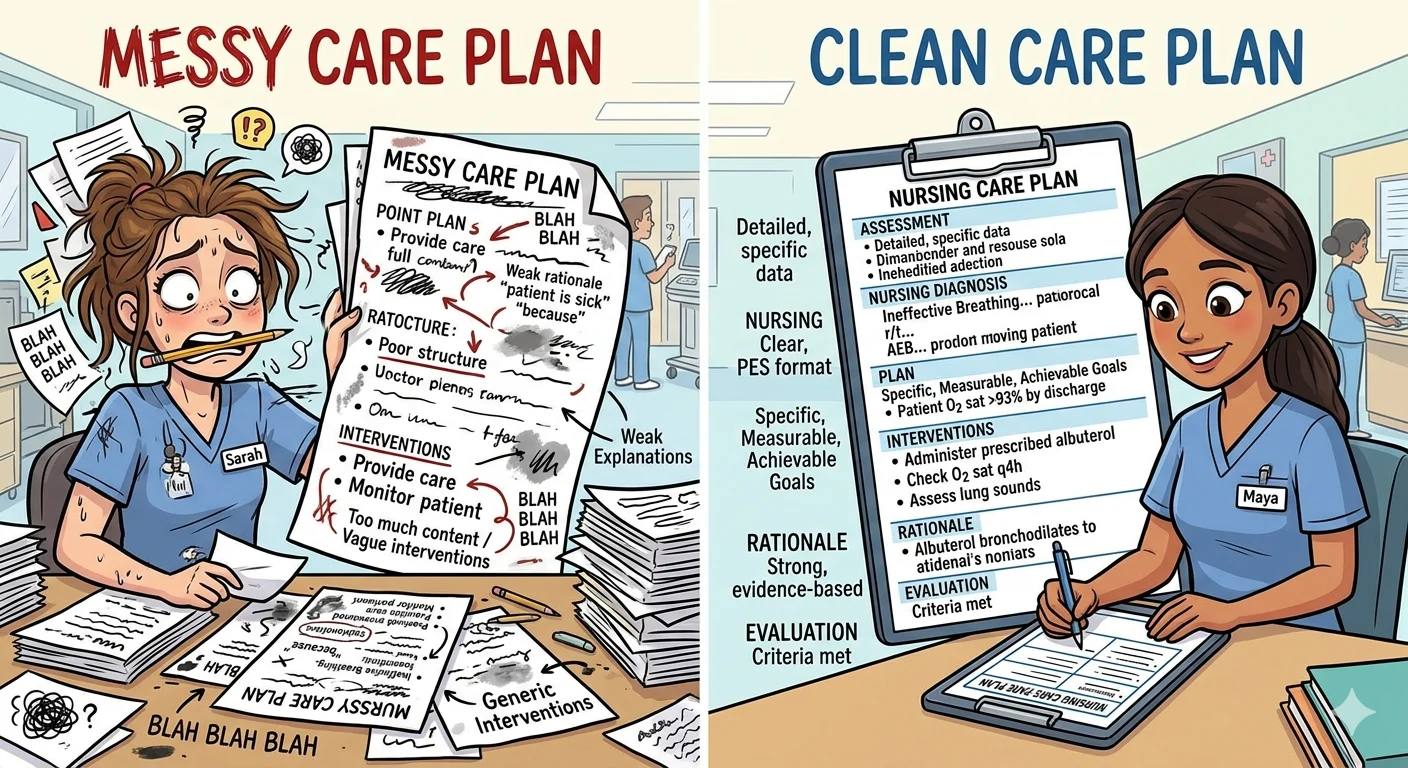
Common Mistakes to Avoid
- Writing too much or too little
- Not explaining reasoning
- Poor structure
- Generic interventions
Tips for Better Marks
- Use simple, clear language
- Organize each section carefully
- Focus on patient needs
- Practice writing care plans
Conclusion
Nursing care plans are easy if you follow the steps:
- Assess
- Diagnose
- Set goals
- Do interventions
- Evaluate
Write clearly, explain your reasoning, and always focus on the patient.
Struggling with Your Nursing Assignment? Get Expert Help Today!
Don’t let deadlines stress you out. Our team of UK-qualified nursing experts will help you:
- Write structured, evidence-based assignments
- Apply NMC standards and clinical reasoning
- Achieve better grades with zero plagiarism